-
Home
-
About Us
-
News
-
Venous Foot Pump
Learn moreModern Treatment for Arterial Disease and Prevention of DVT.
The A-V Foot Pump system works with proven Technology. It mimics the natural process of walking with full weight bearing, which significantly improves the venous return as well as the arterial blood supply.
The A-V Foot Pump system is safe, fast and easy to apply. Its implementation in your therapy concept will lead to significant cost savings due to cheaper consumables, faster wound healing and less recurrence of ulcers, providing a better outcome for your patients.
-
IPC/SCD Compression
Learn moreNEW 5 Inch Color LCD DisplayThe Veinoflow SCD NEW 5006 model is the next evolution of SCD Compression. This device features smart compression controls to deliver compression to legs, feet, or both, and to aid in the prevention of venous thromboembolism, deep vein thrombosis, and pulmonary embolisms. It includes a flexible and transportable design, animated alerts with resolution prompts for any error, low noise, ease of cleaning, and a large LCD touch screen display. Learn moreThe Veinoflow SCD 5005 is a simpler version of the SCD 5006.The system applies intermittent pneumatic compression to increase venous blood flow — helping prevent deep vein thrombosis and pulmonary embolism in at-risk patients. The compression garment has three bladders to deliver circumferential, sequential and gradient compression to ensure clearance of the deep veins without risking distal blood trapping.
Learn moreThe Veinoflow SCD 5005 is a simpler version of the SCD 5006.The system applies intermittent pneumatic compression to increase venous blood flow — helping prevent deep vein thrombosis and pulmonary embolism in at-risk patients. The compression garment has three bladders to deliver circumferential, sequential and gradient compression to ensure clearance of the deep veins without risking distal blood trapping.
The Veinoflow SCD 5005 features delivery compression to the leg, foot, and both. It flexible and transportable design is ideal to be moved between patient rooms, or between rooms in a house for home use. Learn more
Learn moreAdvanced Smart Compression System for VTE Prevention
The Veinoflow SCD LBTK-M-I 5001 is an advanced smart compression system designed to aid in the prevention of Venous Thromboembolism (VTE), including Deep Vein Thrombosis (DVT) and Pulmonary Embolism (PE). This system provides compression therapy for the leg, calf, foot, or both, offering foot-only, leg-only, or combined foot and leg/calf compression to enhance blood circulation and reduce the risk of clot formation.
 Learn moreSingle-chamber IPC compressionThe Veinoacc SCD is a efficient, non-invasive, mechanical prophylaxis system intended to decrease Deep Vein Thrombosis (DVT) occurrence. It intended to provide compression of the calf and/or thigh and can be used in dual or single leg mode, offering flexibility and selection.
Learn moreSingle-chamber IPC compressionThe Veinoacc SCD is a efficient, non-invasive, mechanical prophylaxis system intended to decrease Deep Vein Thrombosis (DVT) occurrence. It intended to provide compression of the calf and/or thigh and can be used in dual or single leg mode, offering flexibility and selection.
Clear audible and visual alarm indicators ensure that the pump always delivers the right pressure. Lightweight, breathable fabric garments ensure comfort and help prevent the build up of heat and moisture.
-
Garments
Learn more3 Chambers Non-Woven Sequential Compression GarmentsThe LBTK 500 Non-Woven Sequential Compression Garments are designed with patient comfort and clinical effectiveness in mind. From durable material to a variety of sizes ranging from small to extra-large for placement on the leg, calf or foot, our garments were carefully engineered to support patients with various needs. Learn more3 Chambers Soft Sequential Compression GarmentsThe LBTK 700 Soft Sequential Compression Garments are designed to address the issue of sweat and heat. Made from cool and soft material to allowing air circulation on the patient’s skin and minimizing sweat pools, irritation and itchiness, our garments are carefully engineered to improve patient acceptance.
Learn more3 Chambers Soft Sequential Compression GarmentsThe LBTK 700 Soft Sequential Compression Garments are designed to address the issue of sweat and heat. Made from cool and soft material to allowing air circulation on the patient’s skin and minimizing sweat pools, irritation and itchiness, our garments are carefully engineered to improve patient acceptance. Learn moreSingle-chamber IPC compression garmentsThe LBTK 600 Lightweight, breathable, latex-free compression garments ensure comfort and help prevent the build up of heat and moisture.
Learn moreSingle-chamber IPC compression garmentsThe LBTK 600 Lightweight, breathable, latex-free compression garments ensure comfort and help prevent the build up of heat and moisture. Learn moreFoot Pad’s directs the impulse against the sole of the foot.LBTK 100 Series Foot Pad’s feature a unique rigid sole, helping to contain and direct the impulse to the bottom of the foot. This helps closely mimic the hemodynamic process that occurs when ambulating. Latex free cushioned Foot Pad’s provides cushioning and maximum coverage of the foot surface area to distribute pressure evenly over the foot and minimize trauma to untreated areas. Minimizes pressure points. Comfortable, cost-effective and environmentally friendly!
Learn moreFoot Pad’s directs the impulse against the sole of the foot.LBTK 100 Series Foot Pad’s feature a unique rigid sole, helping to contain and direct the impulse to the bottom of the foot. This helps closely mimic the hemodynamic process that occurs when ambulating. Latex free cushioned Foot Pad’s provides cushioning and maximum coverage of the foot surface area to distribute pressure evenly over the foot and minimize trauma to untreated areas. Minimizes pressure points. Comfortable, cost-effective and environmentally friendly!
-
VIB Cough-Vest
Learn moreHigh-frequency chest wall oscillation systemThe VIB Cough-Vest airway clearance system is designed to deliver high-frequency chest oscillation to promote airway clearance and improve bronchial drainage. It has been proven to be an effective therapy for a wide range of conditions and when patients use the VIB Cough-Vest system as intended, the changes can be life-transforming. TheVIB Cough-Vest garment’s Velcro like closures, soft touch fabric, and single hose design help simplify your therapy, so you can focus on breathing easier and living better.
-
FAQs
Learn moreVenous thromboembolism (VTE) is a condition in which a blood clot forms most often in the deep veins of the leg, groin or arm (known as deep vein thrombosis, DVT) and travels in the circulation, lodging in the lungs (known as pulmonary embolism, PE). Together, DVT and PE are known as VTE - a dangerous, potentially deadly medical condition.
 Learn more
Learn moreThe acceleration of blood flow and the frequency of compression are the correct criteria for judging the VTE mechanical prophylaxis efficacy,
not its mere garment size! Learn more
Learn moreModern therapy concepts for arterial disease is the key to the successful treatment of related diseases such as chronic wounds and ulcers.
Faster and long-term healing of persistent ulcers.
Significant enhancement of the arterial blood supply.
Active support of the venous function with chronic venous diseases.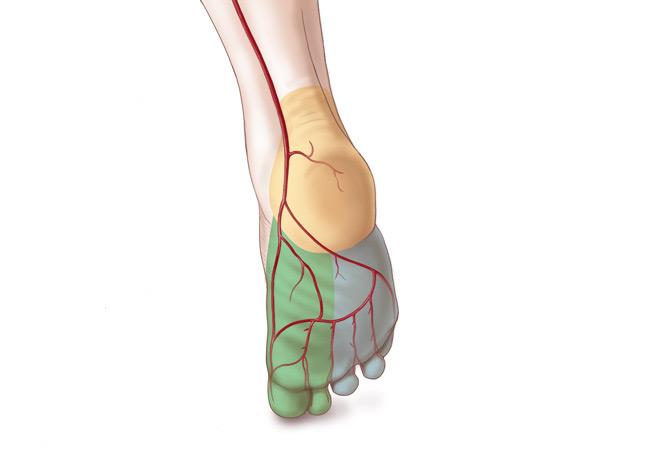 Learn more
Learn moreOur lungs are constantly producing mucus. It is our natural way to keep the lungs clear of infection. In healthy lungs, patients swallow the mucus naturally. When a person is no longer able to effectively clear mucus from their lungs on their own, airway clearance therapy becomes increasingly important to help prevent infection and inflammation.

-
Contact Us
VTE Prophylaxis
Definition and development of VTE
To be able to understand the principles of VTE prophylaxis there are certain definitions you need to be familiar with.
Familiarity with these common terms will assist your understanding why there is a need for VTE prophylaxis.
Deep Vein Thrombosis (DVT)
DVT is also referred to as a blood clot. These occur when red blood cells, fibrin, platelets and leukocytes form a mass within a deep vein, typically of the lower extremities. A blood clot has the potential to break free and travel through the circulatory system to the lungs.
Pulmonary Embolism (PE)
")
PE results when a piece of a blood clot, known as a thrombus, detaches from a vein wall travels to the lungs via the venous network and lodges within the pulmonary arteries. The majority of PE, including fatal PE, are found to have occurred in patients with asymptomatic proximal DVT.
")
VTE Prophylaxis refers to mechanical and pharmocological measures that are taken to prevent DVT and PE.
The following information will provide a brief overview of the role of the circulatory system and the blood components that play a role in clot formation.
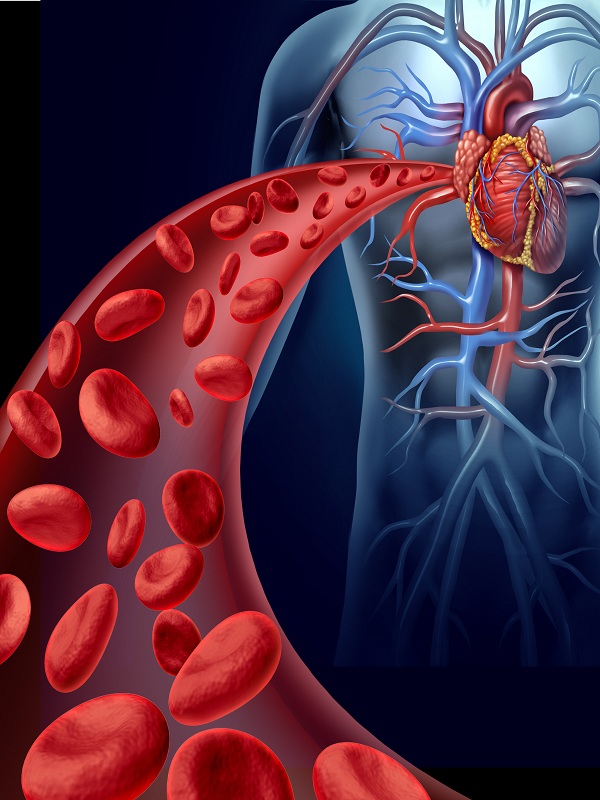
First let’s have a look at the human body’s normal circulation.
")
Blood flowing in the venous system is under lower pressure, and subsequently moves slower than blood flowing within arteries. Blood is therefore more likely to clot in veins than in arteries.
The blood in veins is constantly forming microscopic clots that are routinely broken down by the body. If the balance of clot formation and resolution is altered, significant clotting can occur and a DVT may develop.
Role of platelets in clot formation
As a result of injury to the body, platelets (a type of blood cell) begin to accumulate at the site of injury, then soluble proteins in your plasma (the liquid part of blood) begin to
In normal circulation, oxygenated blood is pumped from the left side of the heart via the aorta to the coronary arteries and other arteries in the body.
Deoxygenated blood returns to the right side of the heart via the inferior and superior vena cava. Blood is then pumped to the lungs, via the pulmonary artery, to pick up oxygen, and then returns to the left side of the heart where the cycle begins again.
It is essential that blood remains fluid during circulation but, in the event of an injury, blood should be able to clot at the site of the injury to maintain haemostasis. However it should not occlude or clot within a blood vessel (arteries or veins).
The feet act as venous foot pumps for the body, the motion of weight bearing while walking activates a range of muscles in the feet and legs which assists in pumping blood to the deep leg veins of the calves.
Contractions of the calf muscles in a normal active person stimulate the flow of blood through the veins of the lower limbs and abdomen towards the heart. Valves are what prevent backflow and pooling of blood within veins.
Clot formation
Blood flowing in the venous system is under lower pressure, and subsequently moves slower than blood flowing within arteries. Blood is therefore more likely to clot in veins than in arteries.
The blood in veins is constantly forming microscopic clots that are routinely broken down by the body. If the balance of clot formation and resolution is altered, significant clotting can occur and a DVT may develop.
Role of platelets in clot formation
As a result of injury to the body, platelets (a type of blood cell) begin to accumulate at the site of injury, then soluble proteins in your plasma (the liquid part of blood) begin to
form fast insoluble fiber’s which act as a mesh to bind platelets and red blood cells together in a soft lump. Typically, the body will dissolve the blood clot after the injury has healed.
The three main factors that cause blood to clot are known as Virchow’s Triad:
")
Venous Stasis
Alterations in blood flow that cause venous stasis include: Varicose veins, immobility, paralysis or fixation devices, laparoscopic surgery and patient positioning during surgical procedures, prior DVT, pregnancy, shock, CHF, obesity, malignancy and increasing age.
Vessel Wall Damage (Trauma)
Damage to the endothelium lining of vein walls occurs with surgery, injury or trauma to a patient, as well with CVC/IV access and treatment with drug irritants. Venous dilatation or distension secondary to administration of anaesthetic agents or extra circulating volume in the body are also known to cause vessel wall damage.
Abnormalities in blood – hypercoagulability
Abnormalities in blood – coagulation changes may be due to numerous risk factors including the following: Anaesthesia, increasing age, dehydration, inflammatory bowel disease, malignancy, polycythemia vera, pregnancy and the puerperium, primary or acquired hypercoagulability, DIC, HIT and hormone therapy.
")
Although DVT may form in any vein, it is more likely to occur in the veins of the lower limbs where blood flow is slower. This may not be life threatening or cause any inconvenience. However it has the potential to result in significant chronic issues, called Post Thrombotic Syndromes. These include: venous ulcers, skin discoloration, pain and swelling.
If a DVT develops, grows large and a thrombus breaks free it can travel through the venous network and eventually reach the lungs. The thrombus can then block the lung vessels causing a serious and potentially fatal PE.
Incidence, cost and risk factors of VTE
International Data
The incidence of VTE related deaths is estimated at 300,000 annually in the U.S with national expenditures on DVT related events estimated at $1.5 billion (Access Economics 2008).
Recent studies from the U.S have listed the top five most prevalent hospital-acquired conditions in terms of cost to the healthcare intitutions as:
· Decubitis ulcers· Postoperative pulmonary embolism and deep vein thrombosis· Accidental puncture and laceration· Post operative respiratory failure· Infections related to medical care.
Together postoperative pulmonary embolism and deep vein thrombosis formed the second most prevalent category and the most expensive, costing a total of $564,000 each year. Both required $15,500 more in care expense per patient.
In the UK and across Europe 45-51 percent of patients undergoing orthopaedic surgery develop DVT. In the UK alone PEs following DVT events, in hospitalised patients, cause between 25,000 and 32,000 deaths each year and it is estimated that across 25 EU countries, approximately 0.7 million DVT and 0.4 million PE events occur each year.
In addition, post-mortems are not routinely performed and therefore VTEs are not always recognised as having been the cause of death.
The need for prevention applies regardless of ethnicity. If VTE prophylaxis is not used, and a patient develops a DVT: they risk associated complications, hospital stay is prolonged, increased drug and laboratory costs occur and potentially fatal PE can eventuate.
VTE risk factors
Most patients have multiple risk factors, which make them more likely to have a VTE event. The more risk factors a patient has, the greater their risk of developing a VTE.
Known risk factors
Risk factors are cumulative; they may be either inherited or acquired.
Known risk factors are listed below and their presence or absence should inform clinical decisions on the use of thromboprophylaxis. The risk factors are grouped into three categories;
1) Individual patient risk factors
· Age (the annual incidence of VTE rises with each decade over the age of forty)
· Pregnancy
· Active or occult malignancy
· Previous VTE
· Varicose veins
· Marked obesity
· Prolonged immobility (prolonged bed rest, immobilisation in a plaster cast/brace, paralysis or prolonged travel)
· Oestrogen-containing hormone replacement therapy or oral contraceptives
· Inherited or acquired thrombophilia.
2) Risks related to an acute medical illness
· Acute or acute on chronic chest infection
· Heart failure
· Myocardial infarction
· Stroke with immobility
· Some forms of cancer chemotherapy
· Acute inflammatory bowel disease
· Risks related to an acute medical illness.
3) Risks related to an injury or surgical procedure
· All surgical procedures increase risk, especially abdominal, pelvic, thoracic or orthopaedic surgical procedures
· Risk is determined by the type of surgery (major joint surgery carries a very high risk, as does surgery for cancer), the type of anaesthesia, the likely duration of immobility (including duration of surgery) and surgical complications
· Leg injury that requires surgery or prolonged immobilisation (NHMRC 2009).
Risk of DVT if no prevention methods are used
If no prevention methods (pharmacological agents or mechanical compression devices) are implemented DVT develops in up to 50% of some categories of hospitalised patients.
Table 1: DVT incidence without VTE prophylaxis
")
VTE Prophylaxis
Evidence-based findings from well designed studies have clearly shown that prevention is possible. With a modest outlay, VTE incidence can be significantly reduced effectively and safely by using specific pharmacological agents and/or mechanical therapies.
Venous thrombosis may lead to pulmonary embolism, post-thrombotic syndrome and recurrent VTE events. Reducing the burden of disease in the hospitalised patient due to VTE requires effective prevention in the form of mechanical and/or pharmacological prophylaxis depending on the patient’s individual risk and associated clinical conditions.
FIRST even before mechanical and/or pharmacological prophylaxis is used, healthcare workers can apply three simple measures as standard practice to prevent VTE.
1. Adequate hydration
2. Gently exercising feet and legs in bed
3. Mobilisation as soon as possible
In combination with these interventions pharmacological and / or mechanical prophylaxis should be utilised where clinically indicated.
Mechanical prophylaxis
The two methods of mechanical prophylaxis options available are;
Intermittent Pneumatic Compression (IPC) or Venous Foot Pump (VFP)
Guide to Selecting the Best Mechanical Prophylaxis
")
Recommended products




- About
- Who We Are
- Venous Foot Pump
- A-V Foot Pump LBTK-M-I 1000
- IPC/SCD Compression
- Veinoflow SCD LBTK-M-I 5006
- Veinoflow SCD LBTK-M-I 5005
- Veinoflow SCD LBTK-M-I 5001
- Veinoacc SCD LBTK-M-I 5004
- VIB Cough-Vest
- VIB Cough-Vest LBTK-K-I 2000 (HFCWO)
- FAQs
- What is Venous Thromboembolism?
- How to select the best VTE Pump?
- Modern Treatment for Arterial Disease
- What is Airway Clearance?
- Contact
- Contact Us